
VNJ Articlesfeaturenursingplan
23 August 2022
Working with nursing care plans- Part 2. Using the nursing care plan by Clare Main
ABSTRACT: Nursing care plans have been used in human medical fields for a number of years and are now moving into use within the veterinary profession. Their two key benefits are: firstly, to ensure all aspects of care are addressed by the practice team and, secondly, to promote good case communication either between different nurses, vets and nurses, and even different clinics. In the author's experience, care plans are fundamental to delivering a good standard of in-patient care. The second part of this series of articles describes the author's personal approach in practice by looking at the use of care plans and how to get started, illustrated by case examples.
How do we use care plans?
There are a number of different elements to this question – who completes the plan, and when; how long is it going to take; and how much detail needs to be included?
Who completes the care plan and when?
This is really important, as there is less benefit from one nurse filling it out on his or her own. The team – often the nurse and vet in charge of the case – should complete it together. Otherwise two nurses can complete it together, especially when they are fully aware of the care needs if they have been involved in the case.
By involving the vet, at least once daily, nurses are empowered to take care of the patient and are aware of the nursing goals. Times to ‘call the vet’ can then also be discussed, so that the nurse knows when he or she might need to do that.
The next most important stage is the updating of that plan. The plan should be flexible and dynamic so that it can be adapted to the changes in the patients needs. Rigid plans that are updated daily may be fine for a very long-stay patient, but are often not appropriate in the initial stages of a patients care. Every time there is a major change is a good time to update it – for example, on recovery from a general anaesthetic, the care plan can be updated to take into account what procedure the pet has just undergone (Care Plan 1).
In any veterinary practice, there will be either shift changes – from the daytime team to the night team, for instance – or even a transfer of that patient to another clinic for out-of-hours care. During these changeovers, the care plan should be re¬worked as part of that process. In that way nothing is missed and messages about such things as ‘what the cat can eat and what it can’t’ can all be updated.
In most practices, this would lead to its being updated two or three times daily. (Care Plans 1, 2 & 3).
Care Plan 1: ‘Nutmeg’ Brown
This cat was involved in an RTA overnight, so the first care plan was done when the cat was transferred from 00H care to the daily care at the practice, taking into account treatments that had already been started OOH. After the veterinary surgeon had examined the cat, a plan was made for the day, including the need for radiographs under general anaesthetic (GAn), a full blood profile, the fluids and pain relief that the cat was receiving and details of owner communication.
A nursing shift change at 11am allows the plan to be updated as the case is handed over, taking into account the normal blood profile and changes in pain relief, but also still raising concerns about bladder function that needs to be especially noted during any radiographs.
After the radiographs have been taken and the cat has recovered from the anaesthetic, the care plan is updated again so that the cat can be transferred to OOH care, and gives the OOH care provider information regarding overall care – for example, are we offering this cat food? What pain relief and medication does she need?
The following morning the whole process starts again, with a review of progress, medication and a plan being made for the day ahead.

Care Plan 2: 'Lucy' Pearce
This dog was in for the day to carry out a 24-hour glucose curve. It was the first time the curve had been done and the dog had been on 6 IU insulin for the past week at home. The first care plan was done when the dog was admitted to the practice, taking into account the owner's report from that morning.


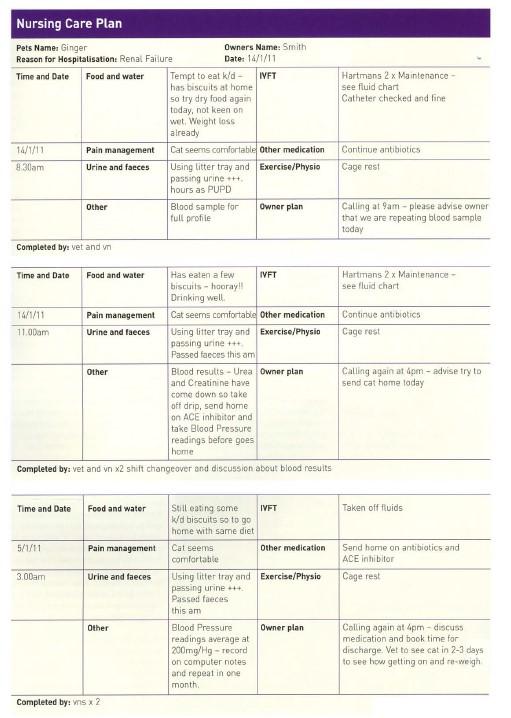
Care Plan 3: ‘Ginger’ Smith
This cat had been diagnosed with renal disease, so he has been admitted and placed on fluids to see if diuresis can reduce the levels of urea and creatinine in the blood. The first care plan was done two days ago, when the cat was admitted, so this is now Day 3 when the practice is planning to repeat the bloods to see if urea and creatinine levels have come down at all. After the veterinary surgeon had examined the cat a plan was made for the day, including the need for another full blood profile, the fluids and concerns about appetite.
A shift change at 11am allows the plan to be updated as the case is handed over, taking into account the lower blood levels of urea and creatinine, but also the fact the cat is to go home on an ACE inhibitor and that a blood pressure measurement today would help to monitor the effectiveness of that drug over time.
At 3pm, the result of the blood pressure monitoring is known and so a plan is made, with particular reference to what the cat needs when he goes home – diet, medication and when he needs to be seen again. This is of particular help to the nurse seeing the cat out. who may not necessarily have been with the cat all day.
How long are they going to take?
With a simple plan the process, only takes around 5 – 10 minutes each time it is updated and this can be done as part of the handover, not in addition. Discussion is one of the most important elements of making these work for the patient and the practice; there is little point in sitting on your own filling in loads of forms if no-one reads them, but going through it together to complete it – or completing it and then running through it with the next person on duty – allows a better understanding of each patient and their needs.
How much detail is needed?
This will vary from practice to practice, from case to case, and which nursing model is used. Having a system whereby each plan has a front page, with more detail about feeding, clinical signs, medication or fluids attached to it, allows the detail to be displayed where it is needed without necessarily cluttering up the main plan. It will also depend on how long the patient is hospitalised and how quickly the condition is changing.
What information do we need?
Most information is about the nursing of the patient’s condition, but some of it needs to be obtained from the owner,
including the pet’s normal toileting arrangements, normal diet and temperament. In an emergency – or if the pet has been transferred from another ‘out-of-hours’ (OOH) clinic – then this information may not immediately be available, but the owner can easily be asked about it all once the pet’s condition is more stable, as in the Case Care Plan 1.
Again, using a nursing model can help put the plan together and determine which information needs to be included.
And finally, how do you get started?
We can see what a nursing care plan might contain, we can refer to various nursing models, and know when and how to use it, but there is often something stopping practice teams and nurses getting started with this process. Every practice really needs to see their benefit by trialling care plans and getting them used as part of the daily routine.
Busy practices have the most to gain as nursing care plans can save time and allow better communication. In smaller practices, where having a pet in, for example on fluids, is not always a daily occurrence, the team benefits from the structure and prompts in a plan. Patients benefit from having their plan regularly updated so those 'all important’ decisions about feeding or pain control are made as part of the daily routine.
Missing ruptured bladders or other hidden injuries and leaving cats on drips without re-assessing their condition for ‘days’ can soon be stopped by the use of regular care planning and care plans (Care Plan 3).
Author
Clare Main BVetMed MRCVS

Clare Main graduated from the RVC, London, in 1992 and spent three years in mixed practice before moving to small animal practice. She joined Hill’s Pet Nutrition in 1998 and worked there for five years before setting up her own practice in 2004 as a joint venture partnership. She is currently working part time in small animal practice and volunteers at the University of Bristol, facilitating communication skills and undergraduate interviews.
To cite this article use either
DOI: 10.1111/j.2045-0648.2011.00053.x or Veterinary Nursing Journal Vol 26 pp 207-211
Useful references
• ORPET & JEFFERY 120061 Moving towards a more holistic approach. VNJ 26(51 May 2006
• JEFFERY 120061 Moving away from the medical model VNJ 21191 September 2006.
• JOINER. T. 120001 An holistic approach to nursing. Veterinary Nursing 15(4] July 2000.
• ORPET. H. 120081 Advances in the Delivery of Practical Nursing Care – practical examples. World Small Animal Veterinary Association World Congress Proceedings. 2008.
• JEFFERY 120081 Advances in the Delivery of Nursing Care – a new concept. World Small Animal Veterinary Association World Congress Proceedings. 2008.
• VOL 26 • June 2011 • Veterinary Nursing Journal